STEMI India’s successful Hub and Spoke model – a blueprint for others?
 With 3 million STEMI cases per year and about 900 cath labs in India, the not-for-profit organisation STEMI India decided, over the last few years, to tackle 2 major issues in the current treatment of STEMI patients – reducing the time delays and selecting the optimal treatment strategy – with the aim to address immediate reduction in mortality and morbidity.
With 3 million STEMI cases per year and about 900 cath labs in India, the not-for-profit organisation STEMI India decided, over the last few years, to tackle 2 major issues in the current treatment of STEMI patients – reducing the time delays and selecting the optimal treatment strategy – with the aim to address immediate reduction in mortality and morbidity.
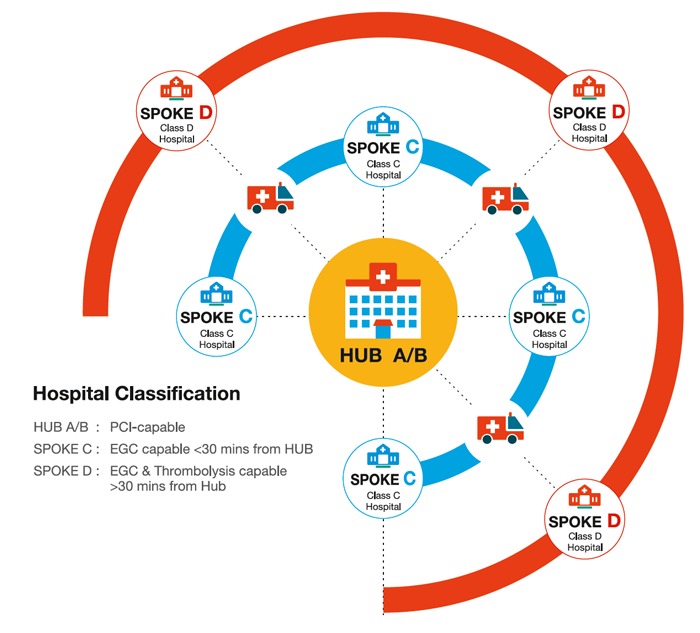
STEMI India chose a dedicated Hub and Spoke model, based on an integrated healthcare network, along with a stringent protocol to address both key problems in the treatment of STEMI through rapid and accurate diagnosis and a resource related choice of the optimal treatment strategy to minimise contact-to-treatment time. This strategy combines pPCI and the pharmaco-invasive strategy of reperfusion according to the location of the patient’s first medical contact.
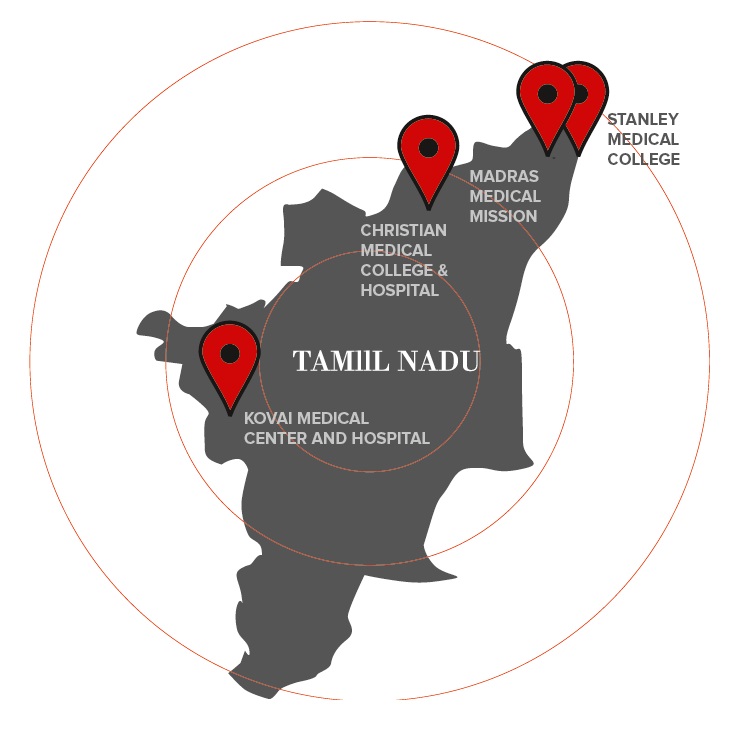
The Hub and Spoke model comprises primary-care health clinics, small hospitals, large tertiary-care facilities and an ambulance network linking all spoke hospitals to the hub. 4 clusters of the Tamil Nadu region were covered by STEMI India’s 1-year pilot project, each one made up of 1 of 2 types of city-based hub hospitals (class A or B) and about 12 to 15 of 2 types of rural spoke hospitals (class C and D) with a network of ambulances connecting these.
A STEMI kit, based on an innovative and affordable technology platform and installed in all ambulances and hospitals, can record and transmit the ECG and other vital signs thanks to a 12-lead ECG monitor coupled with 2G/3G transmission capabilities and GPS functionality. A team of experienced cardiologists is available on-call 24/7 to diagnose the ECG sent to the mobile phone through the STEMI India application installed in all STEMI kits and featuring a proprietary algorithm guiding the physician and paramedics through the STEMI India protocol.
The standardised protocols, developed by STEMI India, aim at prescribing the expected care delivery for a STEMI patient, depending on the setting of care, to meet best practices: pPCI is advocated for patients closed to cath labs with short transportation times to hospital, whereas patients in rural areas and with long transportation times will received the pharmaco-invasive strategy, i.e. thrombolysis followed by pPCI within 3-24 hours of thrombolysis.
The convincing results from the pilot study – greater use of pPCI and pharmaco-invasive strategy vs stand-alone thrombolysis, better access to STEMI care for rural poor population, mortality and MACE reduction – led to a broad range of support for the STEMI India Programme to expand to other Indian states in order to become the model for STEMI management in India.
 Being adaptive to local infrastructure and resources through a modular concept utilizing cloud computing to connect the dots of the network, but stringent in managing medical emergencies by rigorously standardising, the STEMI India model could serve as a blueprint for other Stent-Save a Life! member countries to improve the management of their respective STEMI networks.
Being adaptive to local infrastructure and resources through a modular concept utilizing cloud computing to connect the dots of the network, but stringent in managing medical emergencies by rigorously standardising, the STEMI India model could serve as a blueprint for other Stent-Save a Life! member countries to improve the management of their respective STEMI networks.
Discussions between Dr Thomas Alexander from STEMI India and Stent-Save a Life! are taking place to define how the community could best benefit from such a collaboration. More to follow in the next SSL newsletter…